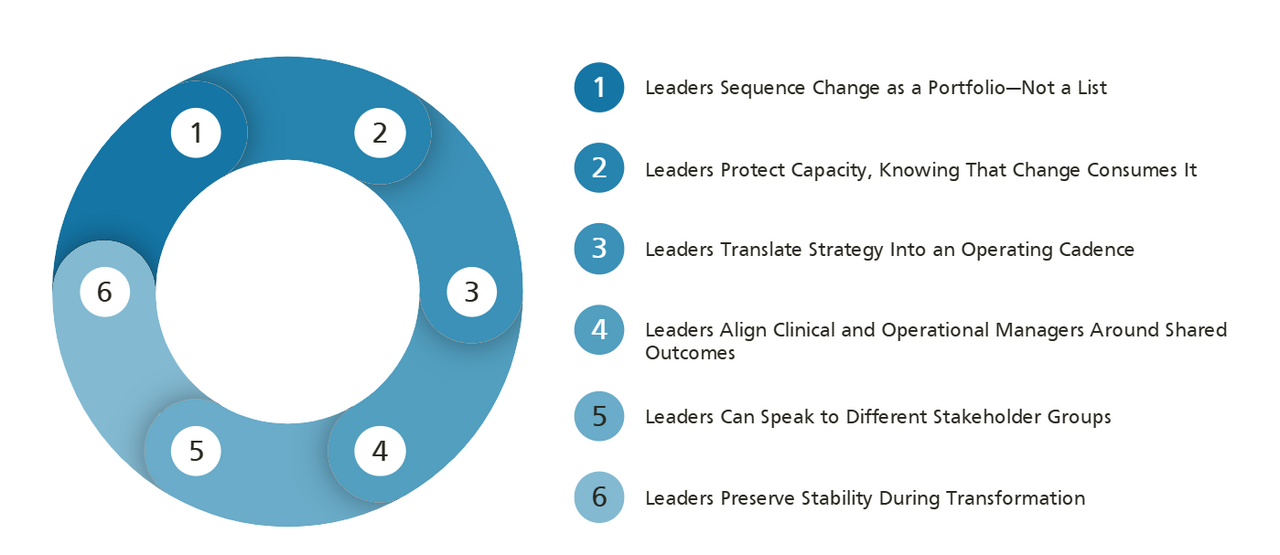
1. Leaders Sequence Change as a Portfolio—Not a List
Leaders who try to execute everything simultaneously overwhelm the system. Effective leaders run transformation like a portfolio of bets with different risk profiles.
A practical sequencing discipline follows a clear logic:
- Stabilize what must not fail: access to care, safety systems, staffing, revenue cycle.
- Transform the workflows that create the most leverage: care coordination, throughput, site-of-care migration, documentation burden.
- Scale what proves effective: standardized playbooks, leadership routines, and governance structures that make the next change easier than the last.
Disciplined execution can protect the front line while the organization builds its capability for sustained change.
2. Leaders Protect Capacity, Knowing That Change Consumes It
The most underestimated constraint in healthcare transformation is bandwidth—clinical, operational, and managerial. Every new initiative draws on the same pool of leadership attention, clinician time, and staff energy.
Leaders who deliver transformation without disruption:
- Quantify change load and track it alongside productivity and quality metrics.
- Build protected time and backfill plans for key roles involved in transformation work.
- Reduce low-value work through automation, simplification, and eliminating redundancies. This supports high-value work and avoids piling new demands onto existing capacity.
This is an area in which interim leadership can serve as a stabilizing lever. In one case, a national healthcare provider navigating a large-scale transformation required urgent stabilization of clinical leadership.
Boyden placed an experienced Interim Chief Nurse to:
- Provide accountability for the nursing and allied health workforce.
- Coordinate with commissioners and care partners.
- Maintain patient care continuity through service redesign.
The interim leader enabled the organization to continue transforming without losing stability in a critical function.
3. Leaders Translate Strategy Into an Operating Cadence
High-performing transformation leaders do not rely on quarterly reviews and steering committees. They build a cadence that is recognizable, measurable, and consistent.
This includes:
- A small number of enterprise-level outcome metrics that span quality, access, cost, experience, and workforce—visible to all leaders.
- Dependency and constraint tracking that identifies where initiatives interact and where bottlenecks are forming before they escalate.
- Weekly and monthly routines that identify trade-offs, force people to make decisions, and maintain accountability.
4. Leaders Align Clinical and Operational Managers Around Shared Outcomes
Healthcare transformation cannot succeed if clinical leaders and operational leaders use different scorecards. Successful leaders build alignment by:
- Defining shared outcomes that relate to both clinical quality and organizational performance.
- Clarifying decision rights so that everyone understands who decides, who advises, and who escalates—especially at the intersection of clinical judgment and operational change.
- Engaging clinicians early in workflow redesign, when they are well-positioned to identify risks and improve design.
When clinicians believe transformation is being forced on them, resistance grows and risk rises. When they believe they are helping to shape it, adoption accelerates. They also are more likely to spot unintended consequences and help to optimize outcomes.
5. Leaders Can Speak to Different Stakeholder Groups
Healthcare transformation leaders work with stakeholder groups that have different priorities, risk tolerances, and vocabularies.
Effective leaders communicate in language that resonates with each audience:
- For clinical leaders: safety implications, workflow impact, evidence, and the "why" behind operational changes.
- For boards: risk profile, financial sustainability, quality trajectory, and governance requirements.
- For frontline teams: what changes, what stays the same, what support is available, and what happens if something goes wrong.
- For regulators and payers: compliance, outcomes data, and alignment with policy objectives.
In Canada, the stakeholder map is especially complex. Leaders must communicate change management with ministries, health authorities, hospitals, clinicians, unions, professional colleges, technology partners, patients, caregivers, and communities.
James Stonehouse notes “the effective leader knows how to gauge the receptor sites of diverse stakeholders, always attuned to their differentiated needs. Where you sit depends upon where you stand.”
6. Leaders Preserve Stability During Transformation
In healthcare transformation, reliability cannot be sacrificed for innovation. Leaders build continuity into transformation design from the beginning:
- Clear escalation pathways for patient safety concerns.
- Contingency staffing and monitoring plans during workflow changes.
- Phased rollouts with explicit go/no-go criteria—and genuine willingness to pause or roll back when signals warrant it.
- Communication protocols that keep frontline staff informed and equipped to flag concerns without fear.
This is how healthcare organizations avoid the most damaging outcome: a transformation that delivers short-term metrics improvement while quietly degrading the trust, safety culture, or workforce stability that sustains the organization over time.